Should Medication Refusal Be Recorded On A Mar Chart
Hey there, curious minds! Ever wonder about the little details that keep things running smoothly in the world of healthcare? You know, those seemingly minor things that actually play a huge role in making sure everyone's safe and sound? Well, today we're diving into one of those intriguing questions: Should medication refusal be noted on a MAR chart?
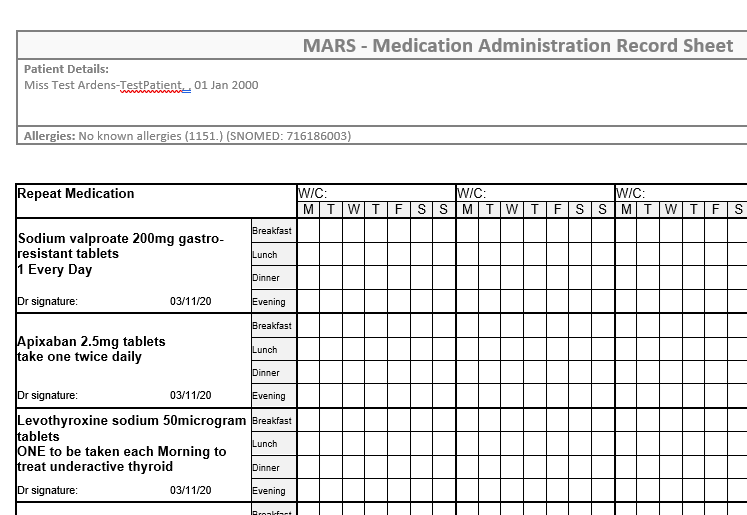
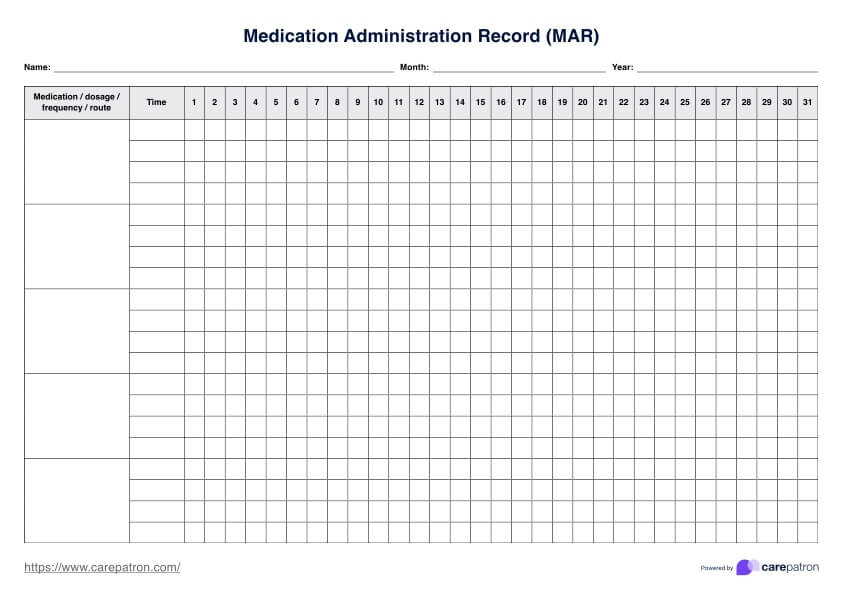
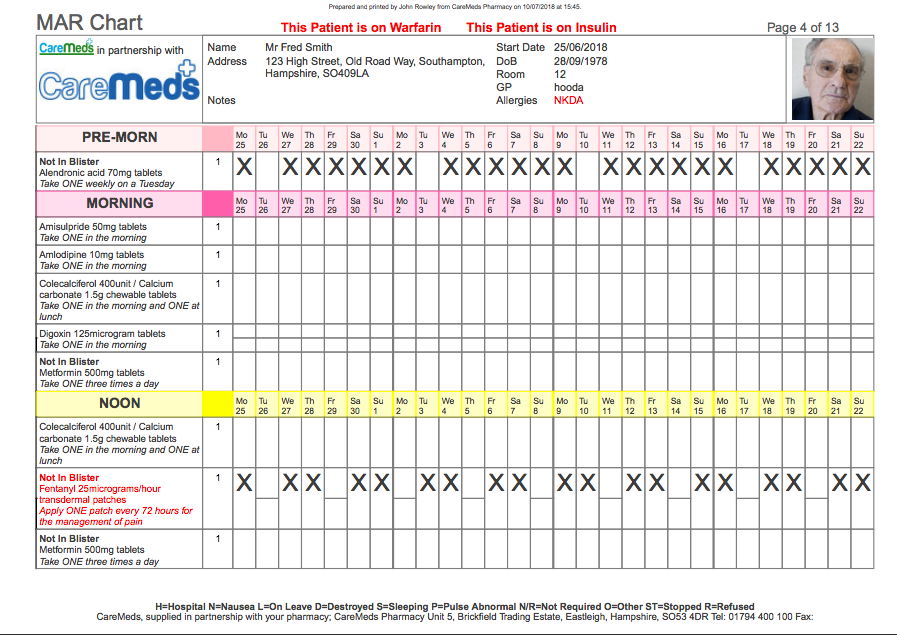
Now, if you're not quite sure what a MAR chart is, don't sweat it! Think of it like a super-important logbook for medications. MAR stands for Medication Administration Record. It’s where nurses and healthcare professionals meticulously track every single dose of medicine given to a patient. It’s basically the patient's medication diary, ensuring they get what they need, when they need it, and that nothing gets missed.
So, the big question is: if a patient says "Nope, not today!" to their prescribed medication, should that "no" be written down in this important log? It might seem like a simple "yes" or "no" situation, but let's unpack it a little, shall we? It’s more than just ticking a box; it’s about understanding the whole picture of a patient's care.
Why It’s Kind of a Big Deal
First off, let's think about patient autonomy. This is a fancy term that basically means every person has the right to make their own decisions about their health, even if those decisions seem a bit… well, quirky to someone else. This includes the right to refuse treatment, even if it's a medication that a doctor believes is essential.
Imagine you're feeling a bit under the weather, and you've got a prescription for some medicine. Now, imagine you just really don't want to take it. Maybe it tastes yucky, maybe you're worried about side effects, or maybe you just have a gut feeling it’s not right for you at that moment. Your doctor might explain why they think it's important, but ultimately, the choice is yours. It’s your body, right?
Recording a medication refusal on the MAR chart is like saying, "We hear you. We respect your decision." It shows that the healthcare team isn't just blindly pushing pills. They're actively engaging with the patient, understanding their concerns, and documenting their choices. This is super important for building trust and a good relationship between the patient and their caregivers.
The Ripple Effect of "No"
So, what happens when a refusal is documented? Well, it triggers a chain reaction, a bit like dropping a pebble into a calm pond. That documented refusal isn't just a dead end; it’s an invitation for further conversation and assessment.
The healthcare team, seeing that refusal, would naturally want to understand why. Is it a temporary thing, like a bad taste in their mouth? Or is it a deeper concern about the medication itself? This opens the door for a much-needed chat. Maybe the nurse can explain the medication in a different way, address fears about side effects, or even suggest alternative ways to administer it if that’s an option.
It’s like trying to solve a puzzle. If a piece isn’t fitting, you don’t just force it. You look closer, you try to understand the shape of the missing piece, and you explore other options. Recording the refusal allows the team to see that there's a piece missing and to start the process of figuring out how to fill that gap.
Think of it like this: if you’re trying to bake a cake and you realize you’re missing eggs, you don’t just carry on and hope for the best. You stop, you check your recipe, and you figure out your next step. Documenting a medication refusal is that crucial "stop and check" moment in the medication administration process.
Keeping Everyone Safe and Sound
Beyond respecting patient wishes, documenting refusals is also a cornerstone of patient safety. This might sound a bit counterintuitive, right? How can saying "no" keep someone safer? Well, let's break it down.
Firstly, it prevents accidental re-administration. If a refusal isn't documented, another caregiver might come along later and, not knowing the patient has already refused, try to give the medication again. This could lead to the patient receiving a double dose, which can be really dangerous. It’s like accidentally putting salt instead of sugar in your coffee – you’d be pretty surprised (and probably not happy!) the second time you tried to drink it.
Secondly, it helps identify patterns. Is the patient consistently refusing a particular medication? If so, this could signal a more significant issue. Perhaps the medication isn't effective, or it's causing an adverse reaction that the patient might not be able to articulate clearly. By documenting these refusals, healthcare providers can spot these trends and investigate further. It’s like a detective noticing that the same suspect keeps appearing at the scene of different, but related, crimes.
This documentation also plays a role in the continuum of care. When a patient moves between different healthcare settings – say, from a hospital to a rehabilitation center, or back home with home care services – a clear MAR chart is essential. If a refusal is documented, it ensures that the new care team is aware of the patient's preferences and past experiences, preventing them from making the same "mistakes" or having to re-educate the patient from scratch.
The "Why" Behind the "No" Matters
So, it’s not just about jotting down "refused." It’s about the context surrounding that refusal. Was it a conscious decision based on informed consent? Was the patient confused or unable to make a decision at that time? Was it a refusal due to religious beliefs, personal values, or a misunderstanding of the medication?
Recording the reason for refusal, as much as can be ascertained, is invaluable. It provides crucial context for the healthcare team. If a patient refuses a blood thinner because they're worried about bleeding, that’s different from refusing it because they believe it’s witchcraft. Understanding the 'why' allows for targeted interventions and education.
It’s like having different keys for different locks. A general "refused" is a basic key, but knowing the reason is like having the specific, intricate key that unlocks the full understanding of the situation. It helps tailor the approach, ensuring that the patient receives the most appropriate and respectful care possible.
In Conclusion: A Little Note Goes a Long Way
So, to circle back to our original question: Should medication refusal be recorded on a MAR chart? The answer, from most healthcare perspectives, is a resounding yes!
It’s about respecting the individual’s right to choose. It’s about ensuring clear communication and preventing errors. It’s about fostering a collaborative approach to healthcare where the patient’s voice is heard and valued. It’s about keeping everyone safe and making sure that the care provided is as effective and personalized as possible.
Think of it as another important piece of the patient’s story, a story that is constantly being written. Every decision, every interaction, and yes, even every refusal, contributes to that narrative. And documenting it ensures that the story is told accurately, compassionately, and effectively, for the well-being of the patient above all else.
It's a small act, writing down a refusal, but the impact it can have on a patient's care journey is truly significant. Pretty neat, huh?