What Is A Risk Assessment In Health And Social Care
So, picture this. I was at my Nan’s house the other day, and bless her cotton socks, she’d decided to rearrange her entire living room. Now, for most people, this is a fun weekend project, right? Maybe a bit of a dust-up. But for my Nan, who’s pushing ninety and has a bit of a wobble when she walks, this involved a perilous dance with a very heavy armchair and a precarious stack of old photo albums. It was like watching a really slow-motion, slightly less dramatic episode of 'The Great British Bake Off,' but with more potential for bruised shins.
I walked in, and there she was, mid-heave, muttering about how the feng shui just wasn’t right anymore. I swear, the armchair wobbled, a teacup teetered on the edge of a side table… it was a symphony of potential household disasters. My first thought, naturally, was, “Oh crumbs, what if she falls?” And then, almost immediately after, “Why on earth is she doing this without asking for help?” It was a moment that, in its own little way, perfectly sums up what a risk assessment is all about in the world of health and social care. It’s basically looking at situations and thinking, “Okay, what could go wrong here, and what can we do to stop it?”
See, in our day-to-day lives, we do these little mental risk assessments all the time. We look both ways before crossing the road, we check if the milk’s gone off before making a cuppa, we probably avoid walking under ladders (though some people are braver than others, I guess!). It’s about spotting potential hazards and taking sensible steps to avoid them. Simple enough, right? Well, when you bring in the complexities of health and social care, this seemingly simple act becomes a really, really crucial part of ensuring people are safe and well.
So, what exactly is a risk assessment in health and social care? At its heart, it’s a systematic process. It’s not just a gut feeling, though those are important too. It’s a structured way of identifying potential dangers, figuring out how likely they are to happen, and then deciding what measures to put in place to either get rid of the danger entirely or at least reduce the risk to an acceptable level. Think of it like being a detective, but instead of solving a crime, you’re preventing one… or, you know, preventing a fall, an infection, or a bad reaction.
The Big Picture: Why Bother With Risk Assessments?
You might be thinking, “Isn’t this all just common sense?” And to a degree, yes. But in health and social care, the stakes are just so much higher. We’re dealing with individuals who might be vulnerable, who might have complex needs, and whose well-being is paramount. Leaving things to chance, or relying solely on instinct, simply isn’t good enough. We need a robust system that ensures everyone involved – the person receiving care, their family, and the care professionals – has a clear understanding of what the potential risks are and how they are being managed.
One of the main reasons we do risk assessments is to protect people. It sounds obvious, doesn’t it? But sometimes, in the hustle and bustle of providing care, it’s easy to overlook a potential problem. A risk assessment forces us to pause, to look critically at a situation, and to proactively identify anything that could cause harm. This could be anything from the physical environment (like uneven flooring at home or poorly maintained equipment in a care facility) to the personal care needs of an individual (like their mobility, cognitive abilities, or specific health conditions).
Another huge part of it is about empowerment and dignity. Now, I know what you might be thinking: “How can assessing risks be empowering?” Bear with me. When a risk assessment is done properly, it should involve the person receiving care as much as possible. It’s not about dictating to them what they can and can’t do. It’s about understanding their wishes, their preferences, and their goals, and then working with them to find ways to achieve those things safely. If my Nan wanted to rearrange her living room, a good risk assessment would have involved a chat with her, understanding why she wanted to do it, and then figuring out the safest way to achieve her goal. Maybe it would have involved her younger (and less wobbly) neighbour helping out, or moving things in stages when she felt up to it. It’s about enabling independence where possible, not removing it.
And let’s not forget legal and ethical responsibilities. As professionals in health and social care, we have a duty of care. This means we are legally and ethically obligated to take reasonable steps to prevent harm. A well-documented risk assessment is a vital piece of evidence that shows we have met this obligation. It demonstrates that we’ve thought about potential issues, assessed them, and put measures in place. It’s not just about covering our backs, though that’s a nice side effect; it’s about genuinely providing the best possible care.
The Building Blocks: What Goes Into a Risk Assessment?
So, how do you actually do one of these things? It's not rocket science, but it does involve a few key steps. Think of it as a bit of a checklist, but a dynamic and person-centred one.
1. Hazard Identification: What Could Go Wrong?
This is the brainstorming phase. You’re looking at a specific situation, an activity, or an environment, and you’re asking yourself: “What are all the things that could potentially cause harm?” This requires a bit of imagination and a good understanding of the person you’re assessing.
For example, if you’re assessing someone’s home for domiciliary care, some obvious hazards might be:
- Trips and falls: Loose rugs, cluttered walkways, uneven flooring, poor lighting. (Sound familiar, Nan’s living room?)
- Fire hazards: Faulty electrical appliances, unattended cooking, smoking materials left accessible.
- Infection control: Lack of handwashing facilities, improper food storage, inadequate cleaning practices.
- Medication errors: Incorrect dosages, forgotten doses, taking medication at the wrong time, or interactions between different drugs. (This is a biggie, and a really common one.)
- Falls from height: Reaching for items on high shelves, using unstable chairs to stand on. (Again, Nan, I’m looking at you.)
- Access and egress: Difficulty getting in and out of the property, especially for individuals with mobility issues.
But it’s not just about the physical stuff. You also need to consider psychological and emotional hazards. Is the person experiencing loneliness? Are they feeling anxious or depressed? Are they at risk of abuse or neglect? These are just as important as a slippery bathmat.
2. Risk Analysis: How Likely Is It, and How Bad Would It Be?
Once you’ve identified a hazard, the next step is to analyse the risk. This involves two main questions:
- Likelihood: How likely is it that this hazard will actually cause harm? Is it something that happens every day, or is it a rare possibility?
- Severity: If the hazard does cause harm, how serious would that harm be? Would it be a minor inconvenience, a serious injury, or something life-threatening?
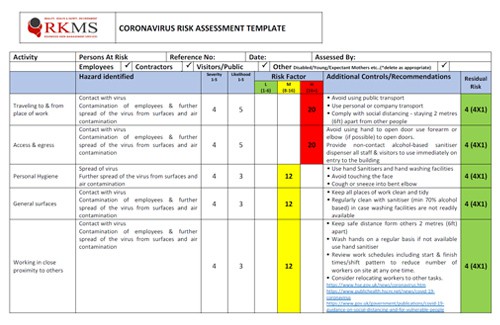
You’ll often see this represented on a matrix, with likelihood on one axis and severity on the other. This helps you prioritize. A hazard that is highly likely to cause severe harm is obviously a top priority. A hazard that is unlikely to cause minor harm might be noted but might not require immediate, drastic action.
For instance, the risk of Nan tripping on a rug is probably quite high given her wobble. The severity could range from a minor stumble to a broken hip. Compare that to the risk of a meteor strike in her living room – extremely low likelihood and probably not something to lose sleep over (unless you live in a very specific part of the universe!).
3. Risk Evaluation: Is the Risk Acceptable?
This is where you make a judgment call. Based on your analysis, is the current level of risk acceptable? In health and social care, the goal is generally to reduce risks to a level that is as low as reasonably practicable (ALARP). This means you can’t eliminate all risk, but you can take sensible steps to minimise it.
If the risk is deemed unacceptable, or if there’s a simple and effective way to reduce it further, then you move on to the next step.
4. Risk Control: What Are We Going To Do About It?
This is the action phase! Based on your evaluation, you decide on the measures you’re going to put in place to control the identified risks. These measures can fall into a few categories:

- Elimination: Can we get rid of the hazard altogether? (For Nan, this might be removing the armchair entirely, though that’s unlikely to go down well!)
- Substitution: Can we replace the hazardous thing with something safer? (Maybe using a lighter, more manoeuvrable chair?)
- Engineering Controls: Can we put physical barriers or changes in place? (Non-slip mats, improved lighting, grab rails in the bathroom.)
- Administrative Controls: Can we change how people work or what procedures are followed? (Developing clear care plans, providing training, establishing routines for medication management.)
- Personal Protective Equipment (PPE): This is usually the last resort, but it can be important. (Gloves for infection control, or perhaps even a mobility aid for the person receiving care.)
Crucially, the control measures should be practical, achievable, and importantly, agreed upon with the person receiving care (wherever possible). It’s no good having a fantastic control measure if the person refuses to use it or finds it too difficult. This is where the partnership aspect really shines.
5. Recording and Review: Keeping an Eye on Things
A risk assessment isn’t a one-off event. It needs to be written down, so everyone involved knows what the risks are and what the control measures are. This record is important for accountability and for continuity of care. And then, the most vital part: review.
Risks change. People change. Situations change. A care plan that was perfect six months ago might be completely inadequate today. Therefore, risk assessments need to be reviewed regularly, and also whenever there’s a significant change in the person’s condition, their environment, or the care they are receiving. Did the new medication have side effects? Has the person’s mobility improved or declined? Did Nan actually manage to move that armchair herself without incident? These are the kinds of things that trigger a review.
Beyond the Checklist: Making It Person-Centred
Now, I’ve broken it down into steps, and it might sound a bit like a bureaucratic exercise. But the absolute golden rule of risk assessment in health and social care is to keep the person at the centre of everything. It’s not about ticking boxes to satisfy an inspector; it’s about genuinely understanding the individual and supporting them to live their life as fully and safely as possible.
This means asking questions like:

- What does the person want to achieve?
- What are their concerns?
- What are their strengths and capabilities?
- What support do they already have in place?
- What are their preferences for how risks are managed?
Sometimes, a person might be willing to accept a higher level of risk in exchange for greater independence or the ability to do something that is really important to them. Our job isn’t to remove all risk, but to help them understand those risks and make informed choices. It’s a delicate balance, and it requires a lot of good communication and trust.
Think about someone who wants to continue gardening, even though they have mobility issues. A risk assessment wouldn’t just focus on the risk of falling while bending. It would explore how they can continue gardening safely. Could we get them a raised garden bed? A kneeling stool with handles? Perhaps involve a volunteer to help with heavier tasks? It’s about finding solutions that enable them to enjoy their hobby, not just stopping them from doing it.
The Irony: When Risk Assessments Get It Wrong
And yes, sometimes, despite everyone’s best efforts, things can still go wrong. And that’s where the review process becomes even more critical. It’s not a failure to learn from what happened. In fact, a good learning culture in health and social care means that when incidents do occur, they are reported, investigated, and used to improve future risk assessments and care practices.
There’s a bit of irony in the whole thing, isn’t there? We’re trying so hard to manage and minimise risk, and yet, the very act of living involves taking risks. My Nan’s armchair saga is a perfect, low-stakes example. She was taking a risk to achieve something she wanted. The risk assessment’s job isn’t to prevent her from wanting to move the armchair, but to ensure that if she does decide to move it, she does so in a way that minimises the chance of her getting hurt. And if she can’t do it safely, then the assessment should lead to finding a safe alternative way to achieve her goal.
Ultimately, a risk assessment in health and social care is a dynamic, ongoing process that underpins safe, effective, and person-centred care. It’s about being proactive, thinking critically, and working collaboratively to ensure that individuals can live their lives with dignity, independence, and the best possible protection from harm. Now, if you’ll excuse me, I’m off to check on Nan… and maybe discreetly slide a few non-slip mats around her living room.